
Douglas R. Lowy
National Cancer Institute

John T. Schiller
National Cancer Institute
The 2017 Lasker~DeBakey Clinical Medical Research Award honors two scientists whose technological advances enabled the development of human papillomavirus (HPV) vaccines, which prevent cervical cancer and other tumors. Douglas R. Lowy and John T. Schiller (both from the National Cancer Institute) took a bold but calculated approach toward a major public-health problem whose solution required them to vault formidable hurdles. They devised a blueprint for several safe and effective vaccines that promise to slash the incidence of cervical cancer and mortality, the fourth most common cancer among women worldwide, as well as other malignancies and disorders that arise from human papillomaviruses.
Cancer-causing microbes
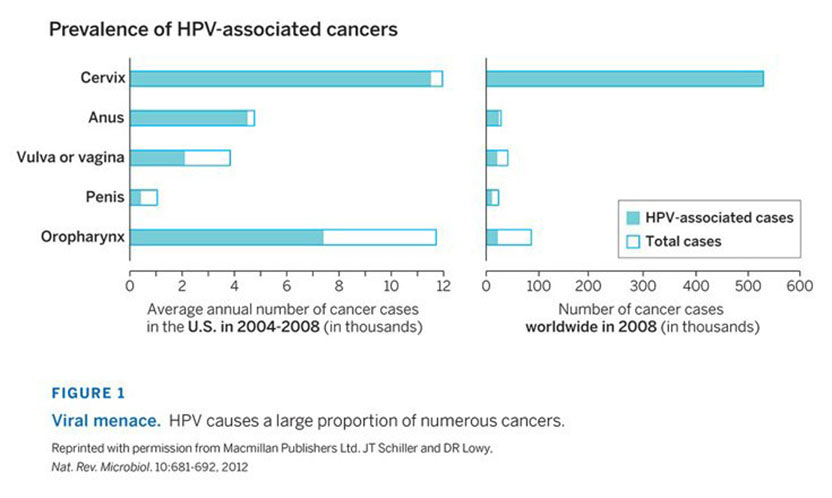
More than 500,000 new cases of cervical cancer are diagnosed annually, and each year, more than 250,000 women die from the malignancy. In the 1980s, Harald zur Hausen (2008 Nobel Prize in Physiology or Medicine) linked the disease to infection with certain types of HPV. Two of them—HPV16 and 18—give rise to about 70 percent of cases, and approximately ten additional types account for the vast majority of the remaining 30 percent. HPV16 and 18 plus these other “high-risk” HPVs also underlie many cancers of the vulva, vagina, penis, anus, and throat (Figure 1). Different HPV family members cause genital warts.
Sexual activity transmits these viruses, and infections usually clear spontaneously. Some persist, however, and high-risk HPVs harbor oncogenes, whose activity can lead to unrestrained proliferation of host cells. The process of transforming normal cells into cancerous ones typically takes at least 15 years, usually longer. By the early 1990s, scientists realized that a vaccine that blocks persistent infection with dangerous HPV types would bestow substantial public-health rewards.
Crafting a vaccine strategy
Live but crippled viral vaccines have vanquished numerous scourges, such as measles and mumps, but the prospect of unshackling HPV’s cancer-promoting genes in the body was considered too dangerous, even inside a weakened virus. To rouse a protective immune response, therefore, Lowy and Schiller hoped to make vaccines that contained only non-oncogenic pieces of HPV16.
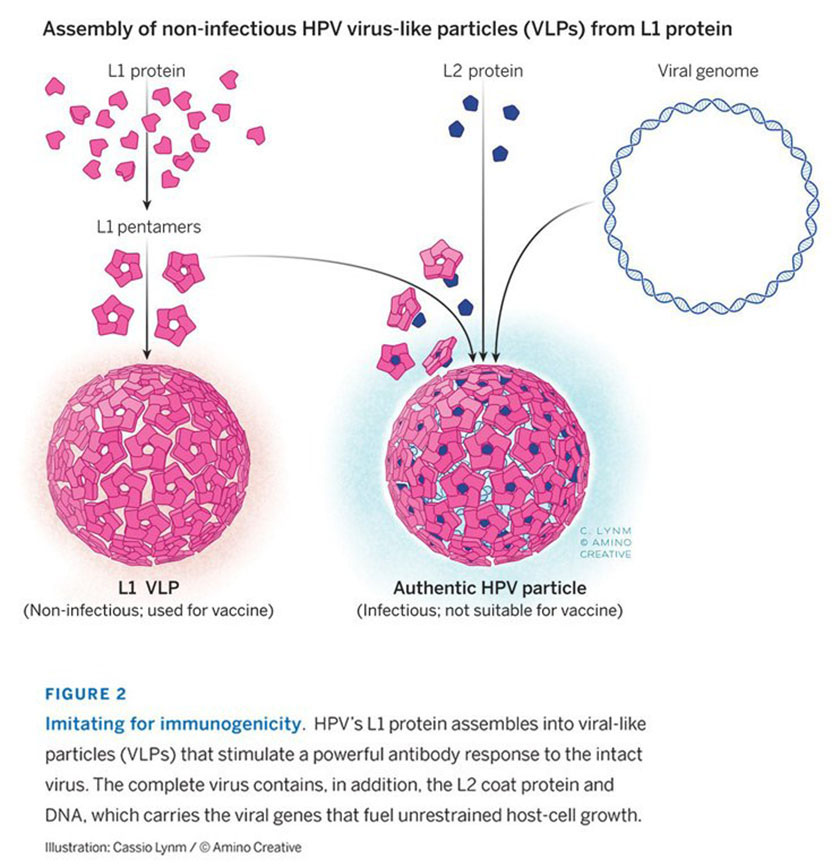
Proteins on the microbe’s surface, L1 and L2, emerged as top candidates because scientists hoped they would behave like coat proteins of other viruses that share HPV’s icosahedral shape. In test tubes, those proteins can arrange themselves into particles whose architecture resembles that of an intact virus. If L1 and/or L2 could similarly self-assemble, the resulting virus-like particles (VLPs) might provide the basis for a vaccine. Because VLPs lack a genome, they would not cause illness; by mimicking HPV’s structure, however, they might prompt a protective antibody response.
In 1991, Ian Frazer (then at Princess Alexandra Hospital, Brisbane, Australia) reported that he could produce HPV16 particles from L1 and L2 together, but not from either one alone. Electron microscopy revealed that the particles were smaller than those of other papillomaviruses, and Frazer presumed they were “incompletely assembled.” He suggested that they might serve as the foundation for a vaccine, but there was no way to test that idea. Unlike the situation for bovine papillomavirus (BPV), which causes cow warts, no experimental system could measure infection by oncogenic human papillomaviruses. Therefore, scientists could not identify agents, such as inactivating antibodies, that prevented HPV16 infection.
Lowy and Schiller wanted to craft a tractable vaccine-development plan. Perhaps, they reasoned, they could create a vaccine against BPV and then transfer its key aspects to HPV. They could use a method that Lowy had developed earlier to quantify BPV infection in lab-grown cells. This choice—and its rationale—proved pivotal for the venture’s success.
In 1991, Lowy and Schiller’s postdoctoral fellow Reinhard Kirnbauer began trying to generate BPV VLPs. The team decided to manufacture viral proteins in insect cells because they churn out bountiful quantities and because the U.S. Federal Drug Administration (FDA) had approved clinical trials of other proteins produced in these cells.
Insect-made BPV L1 assembled into VLPs that resembled authentic BPV particles in appearance and size (Figure 2). Kirnbauer ground up VLP-containing insect cells and injected the mixture into rabbits. Then he tested whether the animals’ blood serum stymied BPV infection of lab-grown cells. Typically, potency is calculated from the degree to which the trial material can be diluted and still curb infectivity. The serum worked so well that Kirnbauer had to repeat the experiment three times before he hit the point at which he no longer detected inhibition—a million-fold dilution.
This exciting observation, reported in 1992, showed that VLPs composed of L1 alone provoke a powerful immune response. However, Lowy and Schiller aimed to foil cervical cancer, not cow warts, so they had to translate their findings to HPV. At first, things did not go well.
Defining assembly characteristics—a defining moment
HPV16 L1, in contrast to BPV L1, assembled poorly. As the researchers scratched their heads, they wondered whether the source of the HPV16 they were using was causing the trouble. It was the standard reference strain in the field, the original isolate that zur Hausen had obtained from a cervical cancer specimen. Cancer cells excel at fostering genetic changes, so perhaps this particular HPV16 had picked up an alteration that compromises its ability to form VLPs, Lowy and Schiller speculated. The team obtained two HPV16 isolates that had come from benign cervical infections rather than cancer and reported in 1993 that their L1 proteins assemble efficiently without L2 proteins. The researchers then identified one particular amino acid in L1 that differed between the original cervical cancer isolate and the non-malignant isolates. This one amino acid was vital to proper assembly.
With a plentiful supply of bona fide HPV L1 VLPs, Lowy and Schiller began trying to stir the interest of commercial vaccine manufacturers. Initial responses were tepid, but in November 1992, when they visited the late Maurice Hilleman (1983 Lasker Public Service Award), a giant in vaccine development at Merck & Co., Inc., he proclaimed that the vaccine would work and Merck would make it. Subsequently, the biotechnology company MedImmune approached the researchers as well. These two companies displayed great courage and dedication in taking on this project, as intensive vaccine programs against other sexually transmitted diseases had failed, and clinical trials to test an HPV preventive would be long and costly.
By mid-1996, several groups, including Lowy and Schiller’s, had established that antibodies against L1 VLPs of rabbit, cow, and dog papillomaviruses avert disease in whole animals. Furthermore, Lowy and Schiller had invented a way to test whether the L1 VLPs they had made from HPV16 could trigger production of virus-inactivating antibodies in lab-grown cells. They used this system to demonstrate that VLPs from genetically normal HPV16—but not the reference version with the assembly defect—induce antibodies that potently inhibit HPV16 infection. Given the evidence that L1 VLPs can impede papillomavirus illnesses and the apparent immunological muscle of the HPV16 L1 VLPs, it was time to test the strategy in humans.
A dream vaccine
Lowy and Schiller, in collaboration with scientists at Johns Hopkins University, conducted the first clinical trial of an HPV16 L1 VLP vaccine, on 36 healthy adults. In 2001, they reported that it was safe and spurred a strong immune response. The following year, researchers at Merck & Co., Inc. and their colleagues published results on the effectiveness of their L1 VLP vaccine, which they tested by assessing whether it could prevent HPV16 infection in sexually active women. None of the almost 800 volunteers who received the vaccine—but 41 of the individuals who received a placebo—developed a persistent cervical infection with HPV16. In contrast, equal numbers of women in the two groups developed potentially precancerous cervical cells caused by HPV types other than HPV16. This observation added weight to accumulating evidence that immunization with one type of HPV VLP provides, at best, limited protection from infection by other types.
Two years later, a team led by GlaxoSmithKline, which had taken over MedImmune’s HPV vaccine program, published a similar study with a vaccine composed of HPV18 as well as HPV16 L1 VLPs. The dual agent prevented persistent infection with the HPV types it represents—and it also thwarted aberrant cell growth that can lead to malignancies.
During the following several years, additional clinical trials confirmed and extended these results with both companies’ vaccines. Merck added HPV6 and HPV11 VLPs to its blend and showed that these components ward off genital warts.
The Merck (Gardisil™) and GSK (Cervarix™) vaccines gained FDA approval in 2006 and 2009, respectively, for prevention of cervical precancer and cancer in women. Gardisil has also been approved to defend against potentially malignant growths of the vulva and vagina, as well as genital warts and anal anomalies in males and females. A second generation Gardisil vaccine that covers five additional high-risk HPV types is also now available.
The lag between HPV infection and cancer diagnosis means that the vaccines’ presumptive ability to reduce malignancies will not become obvious until at least 2030, but their benefits are already evident, especially in countries with strong national vaccination programs. In Australia, for instance, the incidence of genital warts and precancerous cervical abnormalities in young women is plummeting.
By 2015, 47 million women worldwide and 13 million in North America had received a full course of three HPV vaccine doses; an additional 12 million worldwide and 7 million in North America had received one or two. In the U.S., routine HPV vaccination has been recommended since 2006 for girls and since 2011 for boys. By 2015, only 28% and 42% of males and females (age 13-17), respectively, had received at least three HPV vaccinations; 50% and 63% of adolescent males and females, respectively, had received at least one.
Cervical cancer hits developing nations especially hard, largely due to a dearth of screening and treatment programs. Widespread dissemination of the HPV vaccine could drastically shrink that burden. Strong data suggest that a single dose could provide robust protection, and Drs. Lowy and Schiller have spearheaded a large effort that is currently under way to test that proposition. A single-dose vaccination schedule would boost the likelihood of delivering the vaccine’s potential to the world’s poorest inhabitants.
Through creative thinking and problem solving, Lowy and Schiller crafted a foundational strategy that paved the way for pharmaceutical companies to develop vaccines for HPV, a microbe that causes a panoply of life-threatening cancers. The clinical and public health benefits of these innovative efforts are still in an early stage, but the impact has already begun to reverberate across the globe.
by Evelyn Strauss
Key Publications of Douglas R. Lowy
Kirnbauer, R., Booy, F., Cheng, N., Lowy, D.R., and Schiller, J.T. (1992). Papillomavirus L1 major capsid protein self-assembles into virus-like particles that are highly immunogenic. Proc. Natl. Acad. Sci. USA.. 89, 12180-12184.
Kirnbauer, R., Taub, J., Greenstone, H., Roden, R., Dürst, M., Gissmann, L., Lowy, D.R., and Schiller, J.T. (1993). Efficient self-assembly of human papillomavirus type 16 L1 and L1-L2 into virus-like particles. J. Virol. 67, 6929-6936.
Breitburd, F., Kirnbauer, R., Hubbert, N.L., Nonnemacher, B., Trin-Dinh-Desmarquet, C., Orth, G., Schiller, J.T., and Lowy, D.R. (1995). Immunization with virus-like particles from cottontail rabbit papillomavirus (CRPV) can protect against experimental CRPV infection. J. Virol. 69, 3959-3963.
Harro, C.D., Pang, Y.-Y.S., Roden, R.B.S., Hildesheim, A., Wang, Z., Reynolds, M.J., Mast, T.C., Robinson, R., Murphy, B.R., Karron, R.A., Dillner, J., Schiller, J.T., and Lowy, D.R. (2001). Safety and immunogenicity trial in adult volunteers of a human papillomavirus type 16 L1 virus-like particle vaccine. J. Natl. Cancer Inst.. 93, 284-292.
Pastrana, D.V., Buck, C.B., Pang, Y.Y., Thompson, C.D., Castle, P.E., FitzGerald, P.C., Krüger Kjaer, S., Lowy, D.R., and Schiller, J.T. (2004). Reactivity of human sera in a sensitive, high-throughput pseudovirus-based papillomavirus neutralization assay for HPV 16 and HPV 18. Virology. 321, 205-216.
Schiller, J.T., and Lowy, D.R. (2011). Developmental history of HPV prophylactic vaccines Chapter 27. In History of Vaccine Development. Edited by S.A. Plotkin. Springer Publishing Co., New York City, pp. 265-284.
Key Publications of John T. Schiller
Kirnbauer, R., Booy, F., Cheng, N., Lowy, D.R., and Schiller, J.T. (1992). Papillomavirus L1 major capsid protein self-assembles into virus-like particles that are highly immunogenic. Proc. Natl. Acad. Sci. USA. 89, 12180-12184.
Kirnbauer, R., Taub, J., Greenstone, H., Roden, R., Dürst, M., Gissmann, L., Lowy, D.R., and Schiller, J.T. (1993). Efficient self-assembly of human papillomavirus type 16 L1 and L1-L2 into virus-like particles. J. Virol. 67, 6929-6936.
Breitburd, F., Kirnbauer, R., Hubbert, N.L., Nonnemacher, B., Trin-Dinh-Desmarquet, C., Orth, G., Schiller, J.T., and Lowy, D.R. (1995). Immunization with virus-like particles from cottontail rabbit papillomavirus (CRPV) can protect against experimental CRPV infection. J. Virol. 69, 3959-3963.
Harro, C.D., Pang, Y.-Y.S., Roden, R.B.S., Hildesheim, A., Wang, Z., Reynolds, M.J., Mast, T.C., Robinson, R., Murphy, B.R., Karron, R.A., Dillner, J., Schiller, J.T., and Lowy, D.R. (2001). Safety and immunogenicity trial in adult volunteers of a human papillomavirus type 16 L1 virus-like particle vaccine. J. Natl. Cancer Inst. 93, 284-292.
Pastrana, D.V., Buck, C.B., Pang, Y.Y., Thompson, C.D., Castle, P.E., FitzGerald, P.C., Krüger Kjaer, S., Lowy, D.R., and Schiller, J.T. (2004). Reactivity of human sera in a sensitive, high-throughput pseudovirus-based papillomavirus neutralization assay for HPV 16 and HPV 18. Virology. 321, 205-216.
Schiller, J.T., and Lowy, D.R. (2011). Developmental history of HPV prophylactic vaccines Chapter 27. In History of Vaccine Development. Edited by S.A. Plotkin. Springer Publishing Co., New York City, pp. 265-284.
Award presentation by Craig Thompson
Today we honor two exceptional cancer biologists from the National Cancer Institute for their foundational studies that enabled the development of a vaccine to prevent cancer.
Cancer is the disease that people throughout the world fear most for themselves and their loved ones.
Every day we hear of promising new treatments for cancer. Recent winners of the Lasker Clinical Award have helped pave the way for important new treatments for cancer. The discovery of Gleevec for the treatment of chronic myelogenous leukemia put precision medicine on the map and won Brian Druker, Nick Lydon, and Charles Sawyers a Lasker for their work that turned a fatal cancer into a chronic disease. In 2015, Jim Allison was recognized for pioneering studies showing that the immune system could be harnessed to fight cancer. His work launched the exploding array of cancer therapies that seek to augment the immune system rather than damage cancer cells. Together, precision medicine and immuno-oncology offer great hope for cancer patients.
Acceptance remarks
Acceptance remarks, 2017 Lasker Awards Ceremony
It is of course gratifying to be receiving a Lasker Award, but the award is really a tribute to the field of HPV research and to our many colleagues who have contributed to it. More generally, the award highlights the importance of the HPV vaccine as an advance in disease prevention that can overcome the worldwide scourge of cervical cancer and other HPV-associated cancers.
When many people think about recent research achievements in cancer and other diseases, the focus is usually on advances in the treatment of established disease. This attention reflects the drama, satisfaction, and relief that come from a new treatment that can heal sick people whose condition would otherwise not have improved.
Much less attention is generally given to advances that can prevent the development of disease, although these advances may often benefit substantially more people than many advances in treatment. At the risk of oversimplification, I see disease prevention as containing an inherent paradox. On the one hand, the great strength of disease prevention lies in the fact that there are no grateful patients. On the other hand, the great limitation of disease prevention lies in the fact that there are no grateful patients. In both situations, we don’t need to worry about contracting the disease.
For biotech and pharma, the financial incentives for developing interventions that prevent disease usually pale by comparison with those that come from developing interventions that treat established disease. Private philanthropy also tends to focus on treatment. Therefore, the development of most interventions that prevent disease depend on investment by the public sector, just as basic research and research on the causes of disease depend almost entirely on long-term, public sector support.
Development of the HPV vaccine was made possible by sustained public investment in biomedical research by many countries. In the United States, the vast majority of this funding comes from the NIH, which has benefited from strong, bipartisan support from elected officials. Public investment in basic research and in technology development led to identifying HPV infection as the main cause of cervical cancer as well as several other types of cancer. Public investment in disease pathogenesis led to understanding how HPV infection can lead to cancer. And public investment supported the translation of this new knowledge into the technology that enabled the HPV vaccine.
It was at this point that Merck, Medimmune, and GlaxoSmithKline began to develop commercial versions of the vaccine. The vaccine manufacturers took considerable risk, as prior to the HPV vaccine, there was no vaccine that could prevent benign and malignant disease that develops at the initial site of infection. The patient volunteers who participated in the trials also played an indispensable role. Fortunately for everyone, the ability of the commercial vaccines to prevent disease caused by HPV has exceeded even our most optimistic expectations, while also highlighting the value of public-private partnerships in health and disease. Amazingly, eliminating cervical cancer and other HPV-associated cancers as a major public health problem is now a realistic goal.
Acceptance remarks, 2017 Lasker Awards Ceremony
Receiving a Lasker award has prompted me to think a bit more about an individual’s role in moving biomedical research forward. Awards tend to focus on individual scientists, or small group of scientists, whose heads are seen to rise out of the broad stream of the biomedical research enterprise. The question arises “Are the scientists who get these awards the key individuals who channel the stream or is it the stream itself that is primarily responsible for moving the individual scientist forward, such that the those that move the fastest are simply better able to stay in the main flow and avoid bumping into the rocks?”
Although it may seem a bit contrary in this context, I would vote for the stream making the more important contribution. In my estimation, the accumulation of technical and conceptual knowledge in a certain field can combine to make even paradigm shifting discoveries inevitable. For example, does anyone here think that if Harold Varmus and Mike Bishop had become astrophysicists rather than molecular biologists that oncogenes would not have been discovered? Proto-oncogenes are too fundamental to biology to have gone undiscovered. . This is not to diminish the cleverness of their experimental approach, the importance of their discoveries, or the appropriateness of their receiving the Lasker and Nobel prizes. It is my belief that, with rare exception, scientists that rise above their peers do so primarily in recognizing and exploiting the opportunities presented by the current state of the art earlier and faster than others. They function primarily in speeding up the clock of what otherwise would have occurred at a slower pace.
Our own work on HPV vaccines is a good illustration of how prior fundamental accomplishments are the essential precursors to a major advance. For example, without the advent of molecular cloning, the 10 or so HPV types that cause cancer, amongst 100s that don’t, would not have been identified and characterized. Without the development of protein expression systems, we could not have produced the vaccine. Without gene amplification, we would not have had the sensitive assay required for monitoring HPV infection in epidemiological studies that established cancer causation and in the pivotal clinical trials that led to vaccine licensure. None of these critical advances were made with the virus-like particle vaccine in mind. Nevertheless, the fact that 360 copies of a single HPV virion protein can self-assemble into a particle that is incredibly effective at inducing antibodies that block virus infection is such a robust biological phenomenon that it was destined to be discovered given the state of the art at the time.
I would like to leave you with two thoughts about acknowledging the importance of the enterprise over the individual. First, it emphasizes the need for a broad-based approach to funding of both basic and translational research. We can’t pick the winners in advance. And second, relegating the importance of the individual is incredibly comforting in that it implies that major advances in human heath are essentially inevitable if proper resources are devoted to the biomedical research enterprise. So, let’s celebrate the enterprise, as well as the individuals, today.
2016 Clinical Award video
Video Credit: Flora Lichtman
