
Alim Louis Benabid
Joseph Fourier University, Grenoble

Mahlon R. DeLong
Emory University School of Medicine
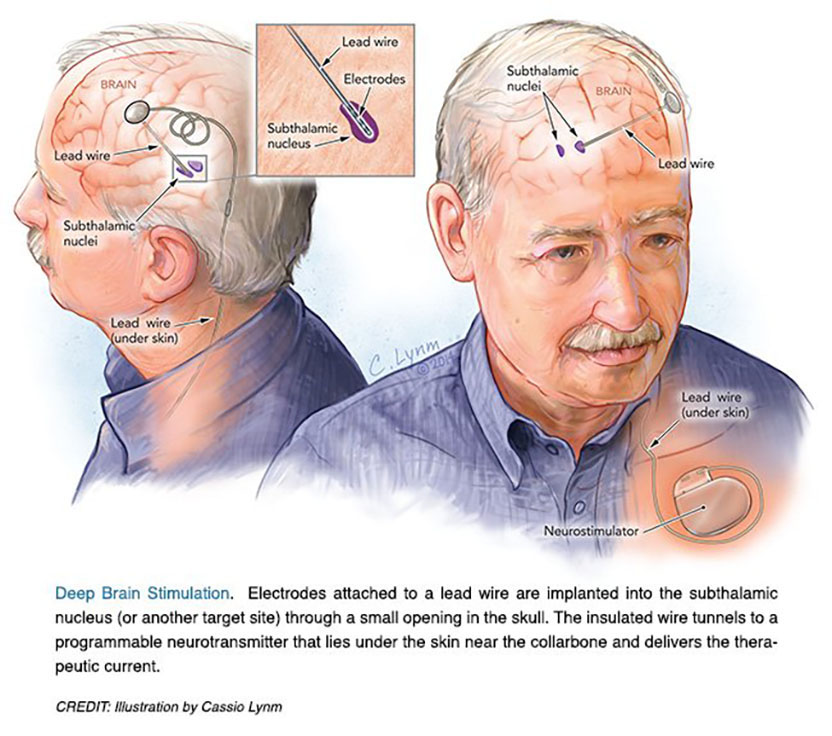
The 2014 Lasker~DeBakey Clinical Medical Research Award honors two scientists who developed deep brain stimulation of the subthalamic nucleus, a surgical technique that reduces tremors and restores motor function in patients with advanced Parkinson’s disease. Mahlon R. DeLong (Emory University School of Medicine) formulated a new model for the brain’s circuitry and exposed a fresh target for this illness. Alim Louis Benabid (Joseph Fourier University, Grenoble) devised an effective and reversible intervention that remedies neuronal misfirings. Their work has culminated in an effective treatment for more than 100,000 individuals worldwide with severe illness who suffer from complications of levodopa therapy.
Parkinson’s disease (PD), perhaps best known for its tremor, slows and stiffens movements. From the 1940s through the 1960s, surgeons battled the ailment by destroying regions of the brain, chosen more by trial and error than by a clear understanding of neural misbehavior. The so-called lesions created by these operations often delivered spectacular and stable effects, counteracting the tremor and, to some extent, other features of PD. Even slight misplacement, however, brought complications rather than benefits. Such damage was permanent, as dead tissue could not be revived.
Provocative pathways
When DeLong began his research, in the late 1960s, the basal ganglia had been implicated in movement, particularly because defects there were associated with illnesses such as PD in which motor disturbances feature prominently. Little was known, however, about how exactly the basal ganglia contribute to movement. To find out, DeLong inserted microelectrodes into monkeys’ brains and measured the activity of specific neurons in the basal ganglia while the animals performed trained actions. He thus matched neurons with tasks; some influenced, for instance, the direction, size, or speed of arm, leg, or facial movements. In this way, he mapped out the organization of the so-called motor circuit.
Based on his own work and that of others as well as existing anatomical information, DeLong proposed a model in which basal ganglia neurons operate in separate circuits. Multiple pathways originate from distinct centers in the cerebral cortex, run through the basal ganglia, and wind up back where they started; the circuits work alongside one another and allow parallel processing of emotions, thoughts, and motor functions.
This work provided insights into the well-established observation that cognitive and emotional problems accompany many motor disorders that stem from basal ganglia failings. Furthermore, the findings supplied a new framework for exploring how basal ganglia components malfunction in various illnesses, including PD. Although dopamine loss clearly causes the disease’s motor perturbations, the associated changes in basal ganglia activities were unclear. DeLong’s model — which included detailed maps of stimulatory and inhibitory signals through the basal ganglia — offered ideas. For example, the final stop in the motor circuit of the basal ganglia is a structure that sends restraining orders onward, thereby suppressing other parts of the motor system. Anything that causes superfluous activity at that site might generate the symptoms that characterize PD.
From addicts to insights
In the early 1980s, sporadic outbreaks of a syndrome that mimics PD started occurring among drug addicts, and scientists traced it to a chemical, MPTP, that was contaminating some batches of “synthetic heroin.” Administration of the compound to monkeys reproduced the key clinical and pathological features of PD, and thus offered a powerful new tool for studying the illness.
DeLong seized upon the opportunity. A part of the basal ganglia called the subthalamic nucleus drives the inhibitory output signal, and in 1987, DeLong reported that MPTP triggers neurons in the subthalamic nucleus of monkeys to fire excessively. Perhaps, DeLong reasoned, the overexuberant signals quash motor activity in PD. If so, inactivating the subthalamic nucleus might ameliorate some of the illness’s worst symptoms.
Next, he did an experiment that would transform PD treatment. He administered MPTP to two monkeys; as usual, they gradually slowed down until they sat motionless, their muscles stiffened, and they developed tremors. DeLong then injected a second toxic chemical that inactivated the subthalamic nucleus. Within one minute, the animals began to move. Gradually, their muscles loosened and the tremors ceased. These findings strongly supported the hypothesis that hyperactivity in the subthalamic nucleus underlies PD symptoms.
High frequency, high hopes
Across the Atlantic, Benabid had also been tackling neurological disorders, and he was frustrated. In a throwback to the pre-L-dopa era, the trickiest patients — those who did poorly with long-term pharmaceutical treatment — would wind up in the operating room. Benabid craved a new tool — something safer that would quiet the most disabling symptoms of PD.
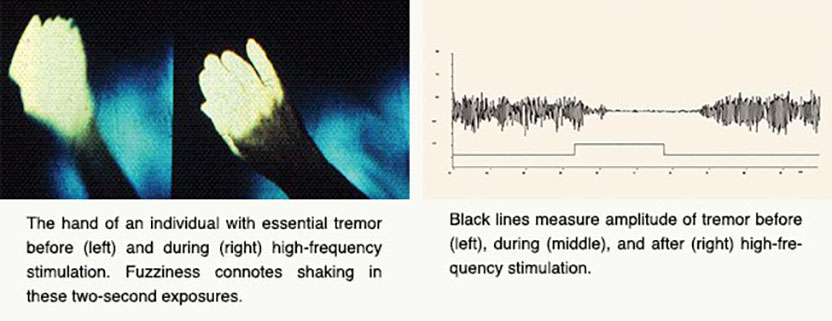
One day in 1987, he was about to create a lesion in a person with essential tremor, a condition that causes trembling in various parts of the body. He was targeting a component of the thalamus that contributes to tremors. As usual, the patient was awake so Benabid could test whether he had located the right tissue; he inserted a probe into the spot that he intended to lesion and sent an electrical pulse to ensure that perturbing this site did not generate undesired effects.
Usually he delivered 50 Hz, but he decided to find out what would happen if he increased the frequency. Just below 100 Hz, something unexpected occurred: The tremor stopped. The patient became so still, Benabid thought that he had caused unintended muscle contraction. He switched off the stimulation and apologized for his mistake. The patient told him not to apologize, as it was the first time in many years that his hand hadn’t shaken.
Benabid repeated the procedure, with the same outcome. Furthermore, when he withdrew the current, the tremor recurred. The effect, therefore, was reversible.
Benabid realized he was onto something exciting. Deep brain stimulation had been used for more than two decades to treat pain, but no one had dialed up the frequency. Later that year, he tried the same approach for PD patients. In addition, he implanted a device that was on the market for pain relief and delivers constant stimulation. Some of the individuals benefited from the procedure, and no complications occurred.
In 1991, Benabid reported that high-frequency stimulation could be deployed bilaterally in people with essential tremor and PD; this strategy reduced tremor on both sides of the body. The gains were long lasting, and adverse effects were mild; furthermore, any undesired outcomes could be reversed by reducing stimulation.
Although the technique quelled tremors, Benabid knew that this symptom was not the one that most debilitated people with PD. Perhaps high-frequency stimulation of brain areas other than the thalamus (i.e., the subthalamic nucleus) would alleviate the more troublesome aspects of the illness such as slowness of movement and rigidity, he reasoned.
In this state of mind, Benabid read DeLong’s report that damage to the subthalamic nucleus wipes out multiple symptoms of PD in animals. This site was not an attractive target: Lesioning procedures and spontaneous lesions had established decades earlier that, when things went wrong, violent flailing could result. By that time, however, Benabid had performed high-frequency stimulation of the thalamus and other brain regions’ in more than 150 patients. He was confident that he would cause no harm in the subthalamic nucleus; if necessary, he could remove the electrode.
In 1995, Benabid reported results from the first humans who received bilateral, high-frequency stimulation of the subthalamic nucleus — three people with severe PD. The treatment suppressed slowness of movement and muscle rigidity.
Eight years later, he confirmed and extended these results in a study of individuals who had undergone the procedure five years earlier. The surgery restored motor skills, suppressed tremor, and improved the ability to conduct normal activities of daily living. Furthermore, people were able to slash their dosage of L-dopa and related medications, which reduced associated complications.
In 2002, the US Food and Drug Administration (FDA) approved high-frequency stimulation of the subthalamic nucleus for treating advanced Parkinson’s disease. The method is not a cure, and it does not reverse all aspects of the malady. In particular, speech and cognition continue to decline.
Many questions remain about the mechanism of this intervention. It might jam or replace inappropriate circuit activity. Regardless how it works, surgeons are using high-frequency deep brain stimulation to combat an ever-growing number of sites and diseases: essential tremor, dystonia — a condition of involuntary muscle contractions — and even psychiatric illnesses. The FDA approved its use for obsessive-compulsive disorder in 2009, and scientists are investigating applications for drug-resistant depression and Tourette syndrome.
Through their open-minded explorations and willingness to challenge dogma, Benabid and DeLong have delivered extraordinary medical innovations to humankind. By reaching deep into the brain, they have soothed some of the most troubling conditions that corrupt it.
by Evelyn Strauss
Key publications of Alim Louis Benabid
Benabid, A.L., Pollak, P., Louveau, A., Henry, S., and de Rougemont, J. (1987). Combined (thalamotomy and stimulation) stereotactic surgery of the VIM thalamic nucleus for bilateral Parkinson disease. Appl. Neurophysiol. 50, 344-346.
Benabid, A.L., Pollak, P., Gervason, C., Hoffmann, D., Gao, D., Hommel, M., Perret, J.E., and de Rougemont, J. (1991). Long-term suppression of tremor by chronic stimulation of the ventral intermediate thalamic nucleus. Lancet. 337, 403-406.
Limousin, P., Pollak, P., Benazzouz, A., Hoffmann, D., Le Bas, J.F., Broussole, E., Perret, J.E., and Benabid, A.L. (1995). Effect on parkinsonian signs and symptoms of bilateral subthalamic nucleus stimulation. Lancet. 345, 91-95.
Limousin, P., Krack, P., Pollak, P., Benazzouz, A., Ardouin, C., Hoffmann, D., and Benabid, A.L. (1998). Electrical stimulation of the subthalamic nucleus in advanced Parkinson’s disease. N. Engl. J. Med. 339, 1105-1111.
Krack, P., Batir, A., Van Blercom, N., Chabardes, S., Fraix, V., Ardouin, C., Koudsie, A., Dowsey-Limousin, P., Benazzouz, A., Le Bas, J.F., Benabid, A.L., and Pollak, P. (2003). Five-year follow-up of bilateral stimulation of the subthalamic nucleus in advanced Parkinson’s disease. N. Engl. J. Med. 349, 1925-1934.
Mallet, L., Polosan, M., Jaafari, N., Baup, N., Welter, M.L., Fontaine, D., du Montcel, S.T., Yelnik, J., Chéreau, I., Arbus, C., Raoul, S., Aouizerate, B., Damier, P., Chabardès, S., Czernecki, V., Ardouin, C., Krebs, M.O., Bardinet, E., Chaynes, P., Burbaud, P., Cornu, P., Derost, P., Bougerol, T., Bataille, B., Mattei, V., Dormont, D., Devaux, B., Vérin, M., Houeto, J.L., Pollak, P., Benabid, A.L., Agid, Y., Krack, P., Millet, B., and Pelissolo, A. (2008). Subthalamic nucleus stimulation in severe obsessive-compulsive disorder. N. Engl. J. Med. 359, 2121-2134.
Key publications of Mahlon R. DeLong
Alexander, G.E., DeLong, M.R., and Strick, P.L. (1986). Parallel organization of functionally segregated circuits linking basal ganglia and cortex. Ann. Rev. Neurosci. 9, 357-381.
Miller, W.C. and DeLong, M.R. (1987). Altered tonic activity of neurons in the globus pallidus and subthalamic nucleus in the primate MPTP model of parkinsonism. In: Advances of Behavioral Biology. M.B. Carpenter and A. Jayaraman (eds.), Plenum Publishing Corp., 32, 415-427, New York.
DeLong, M.R. (1990). Primate models of movement disorders of basal ganglia origin. Trends Neurosci. 13, 281-285.
Bergman, H., Wichmann, T. and DeLong, M.R. (1990). Reversal of experimental parkinsonism by lesions of the subthalamic nucleus. Science. 249, 1436-1438.
Bergman, H.G., Wichmann, T., and DeLong, M.R. (1994). The primate subthalamic nucleus: II. Neural activity in the subthalamic nucleus and pallidum in the MPTP model of parkinsonism. J. Neurophysiol. 72, 507-520.
DeLong, M.R. and Wichmann, T. (2007). Circuits and circuit disorders of the basal ganglia. Arch. Neurol. 64, 20-24.
Award presentation by Greg Petsko
 In 1972, the novelist Michael Crichton, whose Harvard Medical School education seems primarily to have turned him into a techno-Luddite, wrote a novel called The Terminal Man. It told the story of Harry Benson, who has electrodes implanted into his brain to suppress his psychomotor epileptic seizures. The electrodes are controlled by a small computer with a power pack under the skin in his shoulder. Unfortunately, this being a Michael Crichton novel, the technology is flawed and Benson is psychotic, and — well, you can probably guess how this turns out.
In 1972, the novelist Michael Crichton, whose Harvard Medical School education seems primarily to have turned him into a techno-Luddite, wrote a novel called The Terminal Man. It told the story of Harry Benson, who has electrodes implanted into his brain to suppress his psychomotor epileptic seizures. The electrodes are controlled by a small computer with a power pack under the skin in his shoulder. Unfortunately, this being a Michael Crichton novel, the technology is flawed and Benson is psychotic, and — well, you can probably guess how this turns out.
That same year, 1972, a young medical doctor in France named Alim-Louis Benabid became a staff neurosurgeon at Joseph Fourier University in Grenoble while also beginning his studies for an eventual doctorate in physics. And also in 1972, in the United States, another young doctor, Mahlon DeLong, was finishing up his time as a research associate in the National Institute of Mental Health.
Eventually, the work of these two men would coalesce into something strikingly similar, sort of, to the device in The Terminal Man. But its use, Michael Crichton could never have dreamed up: a new therapy for Parkinson’s disease.
Acceptance remarks

Acceptance remarks, 2014 Lasker Awards Ceremony
I was born in France during World War II and raised as a teenager during the Algerian War. My brothers and I were told by my father and my mother that peace was the highest value to pursue. My father, who was an MD, wanted me to be a physician and my mother who was a nurse wanted me to be a physicist. To preserve peace, I had no other choice than being both.
I would say, then, that my life has been a science fiction novel, my story being based on the patient’s problems and expectations, the use of increasingly sophisticated tools in the battles, the thrill of facing challenges, and the delight of solving them, with sometimes happy ends for the patients, and sometimes not.
Every chapter has been an adventure shared with mentors, friends, students. The tempo was made by the goals to reach, the deadlines to meet, and the odds to overcome. Everyone needs to know how much worthwhile are his own achievements. The first and most important reward comes from the patients. Recognition and prizes are the milestones of a career. Some, such as the Lasker~DeBakey Award, are unreachable horizons you dare to dream of, without really believing the dream could become true.
Being considered for the Lasker~DeBakey Award is itself an honor. Being actually awarded is an incredible shock, and the honor this award conveys is even greater when you share it with a scientist and a friend that you respect and admire, such as Mahlon DeLong. I thank you all for your trust and belief and acknowledgement in what I tried to achieve.

Acceptance remarks, 2014 Lasker Awards Ceremony
I don’t recall when I realized I wanted to do research, but I have always enjoyed understanding how things work. A growing fascination with how the brain controls behavior led me to medicine and then to neurology. This took a clear direction when I found a choice research position at the NIH in the laboratory of renowned researcher Edward Evarts. Because the other obvious brain regions were already assigned to other fellows, I was asked to work on the basal ganglia, a cluster of poorly understood brain structures, and to determine their role in the control of bodily movements.
For years I never thought about finding a cure for anything but was fascinated by the progress in understanding the anatomical relations and functions of these mysterious structures. Almost two decades later, a new animal model of Parkinson’s was developed, made possible by the discovery of a toxin that produced clinical features and pathology closely resembling Parkinson’s, resulting from a loss of dopamine in the basal ganglia. Our basic research provided a solid foundation for what was to come. We found abnormal neuronal activity throughout the motor circuit of the basal ganglia and ‘struck gold’ by making a lesion in the subthalamic nucleus, which, by interrupting the circuit, almost immediately restored movement and eliminated tremor and rigidity. Most importantly, the findings provided insight into the neuronal dysfunction responsible for Parkinson’s and a strong rational for surgical intervention as well as a novel target.
Having spent much of my early career in both basic research and clinical work, I have been fortunate to see how the basic science contributes to patient care. I am also aware of how far this field, that we now call neuromodulation, has progressed.
Lasker Awards honor individuals who contribute critically to a research problem — but they also highlight the larger progress in a given field, in our case, using targeted electrical stimulation to restore function in the disrupted neural networks responsible for both neurologic and psychiatric disorders.
For nearly a century, neurologists learned about brain function by correlating the behavioral changes caused by strokes with the damage to specific regions of the brain. With deep brain stimulation, we are now not only able to treat disorders such as Parkinson’s — we’re also able to learn about brain networks and their function by observing the effects of targeted stimulation and activation. Whereas we previously thought about brain ‘centers’, we now focus on specific brain circuits and how they ‘go wrong’ in neurologic and psychiatric disorders. Understanding how neural circuits are disrupted by disease and how lesions and electrical stimulation can improve function is still poorly understood. Understanding brain function and its disorders is the last and most challenging frontier of medicine.
Some of our real progress and ‘breakthroughs’, are made, I believe, serendipitously, while we are doing other things — like just trying to understand how things work. I sometimes wonder whether, in our urgency to find cures, we sometimes omit the basic science necessary to understand how things work — and by doing so, may miss the chance of finding a new treatment.
Over the last 25 years, I mutated not only mouse genes, but changed myself, morphing from a molecular biochemist into a mouse geneticist into an electrophysiologist into a behavioral neuroscientist. These changes gave me the pleasure of always learning something new about how synaptic vesicles and synapses work, although these changes unfortunately have not improved my looks.
The 1990ies were an amazingly thrilling time! During this time, we together with our long-time collaborators Reinhard Jahn and Jose Rizo, and in parallel with Richard Scheller and others, discovered the role of SNARE and SM proteins in synaptic vesicle fusion. We identified synaptotagmins as calcium-sensors in neurotransmitter release, showed how synapses are organized by active zone proteins, and described the first synaptic cell-adhesion molecules that guide synapse formation. These discoveries and conceptual advances were the beginning of an understanding of synapses, which has now become generally recognized. During the course of our work, the studies of Jim Rothman, who received a Lasker Award in 2002 for his work on the cell biology of vesicle fusion, expanded our thinking and injected great enthusiasm into the rapidly growing field of neurotransmitter release.
I thank the Lasker Foundation — I thank you all for giving me this award, and I hope to live up to it!
Interview with Alim Louis Benabid and Mahlon R. DeLong
Video Credit: Susan Hadary
