
Roy Calne
University of Cambridge

Thomas E. Starzl
University of Pittsburgh
The 2012 Lasker~DeBakey Clinical Medical Research Award honors two scientists who developed liver transplantation, an intervention that has restored normal life to thousands of patients with end-stage liver disease. Through their systematic and relentless efforts, Roy Y. Calne (Emeritus, University of Cambridge) and Thomas E. Starzl (University of Pittsburgh) created a medical procedure that most physicians deemed an impossible dream. Some of Starzl’s and Calne’s early patients — originally diagnosed with untreatable and lethal diseases — are still thriving today, decades after their surgeries.
The liver performs many services that are vital for life. It detoxifies harmful substances, manufactures essential materials for the body, stores energy, and secretes bile, which helps digest fats. In the late 1950s, serious liver diseases were fatal, and treatment prospects looked bleak. The idea of transplanting any organ from an unrelated individual seemed foolish to most experts. Rejection — the process in which a body’s immune system attacks unfamiliar tissue — posed a seemingly insurmountable obstacle, and other aspects of liver biology presented overwhelming challenges. This organ supplies clotting factors, and liver disease produces tremendous pressure in the veins, creating a sea of wormlike vessels many times bigger than usual in which a tiny nick can trigger massive blood loss. Patients with liver disease, therefore, bleed extremely easily and often uncontrollably. Furthermore, multiple vessels deliver blood to the liver and drain other substances, so surgical manipulation of the organ is anatomically complicated.
Learning new tricks from dogs
In the late 1950s, a particular feature of liver anatomy captured Starzl’s attention. Two large blood vessels serve this organ, one of which — the portal vein — runs through the gastrointestinal tract and pancreas, picking up substances from those sites. Controversy boiled about whether the nutrient- and hormone-rich portal blood contributes to liver health. To study this question, Starzl developed several liver-transplant procedures and gradually refined them. In 1958, his canine patients began surviving the operation. Although Starzl had not intended the surgery as a step toward human liver transplantation, the work established that the technique was feasible, and he set his sights on bringing it to the clinic.
By 1960, Starzl (then at Northwestern University, Chicago) and the late Francis Moore (Peter Bent Brigham Hospital, Boston) had independently tackled many problems associated with the dog liver replacements. Cutting off the blood supply damages the liver, for instance, so Starzl devised preservation methods: He cooled the donor organ by infusing it with chilled solutions, a practice that is now universal. Both groups also worked out key technical aspects of the operation. For example, when they realized that dogs died from acute heart failure when they clamped two particular veins, they each devised blood-bypass methods that permitted surgical success.
Enter immunosuppression
Despite this progress, skepticism flourished about the utility of any type of organ transplantation. Perfecting an operation from which few would benefit — due to the apparently impenetrable immune barrier between non-identical twins — seemed futile. Nevertheless, a handful of scientists pursued the venture in animals, and between 1959 and 1962, surgeons performed seven initially successful human kidney transplantations. Before their operations, the patients underwent total body irradiation to thwart immune attack.
Interested in the immunological aspects of transplantation, Calne had been studying irradiation in dogs. Because the procedure was extremely toxic, he began testing chemicals that might combat rejection. In 1960, Calne (Royal Free Hospital, London) and, independently, the late Charles Zukoski (Medical College of Virginia, Richmond) deployed a drug, 6-mercaptopurine, that was known to block immune responses to foreign proteins. This agent kept some dog kidney recipients alive for months and demonstrated for the first time that chemical immunosuppressants could fend off rejection. Calne then used 6-mercaptopurine in a few patients and achieved some benefit. Soon afterward, he obtained better results — in dogs — with azathioprine (Imuran), a chemical relative of 6-mercaptopurine. His success inspired Joseph Murray at the Brigham to try it in humans. In 1962, Murray used azathioprine in a kidney transplant patient, who survived for 17 months.
However, when most azathioprine-treated transplant patients did not surpass six months’ survival, enthusiasm plunged in the nascent organ-transplant community. Working with dogs, Starzl made crucial improvements: He began azathioprine before the operation and added the steroid prednisone.
Starzl opened a kidney transplantation program in Denver (University of Colorado), informed by his animal work, and started obtaining excellent outcomes: One of his patients is alive today, 49.5 years after the surgery. He also overturned conventional wisdom about rejection, which held that the process was unstoppable once it started. Starzl decided to proceed with a liver-transplant program, using the dual immunosuppressive regimen he had developed for the kidney.
Launching livers
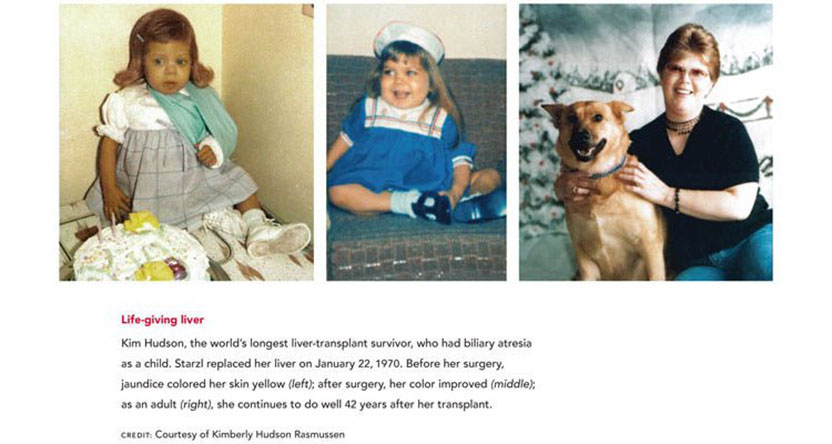
In March, 1963, Starzl attempted the first human liver transplant, on a child with biliary atresia, a condition in which the bile-carrying tubes are blocked. The patient bled to death during the operation. Although the next several liver recipients died within a few weeks after their surgeries, some of them endured long enough to demonstrate that transplanted livers could function.
Surgeons worldwide declared a moratorium on the procedure and analyzed what had gone wrong. The transplanted livers, retrieved at autopsy, showed no signs of rejection — a significant achievement. Instead, bacterial infections, caused in part by the bypass tubing that had been essential for dogs, had killed most of the patients.
During the next few years, Starzl improved the procedure in many ways. He used an antibody, antilymphocyte globulin (ALG) that restrains rejection and demonstrated that portal-vein blood contains substances that keep livers healthy. Until then, experts in experimental liver transplantation had been weighing the merits of adding a second liver rather than replacing the diseased organ. Because supplemental livers were not hooked up to the portal vein, the finding clinched the decision to opt for replacement.
During this period, Calne read that a few unmedicated pig liver recipients survived for a surprisingly long time. This result intrigued him and drew him toward the liver. He subsequently showed that liver grafts in pigs are tolerated better than other transplanted tissue, an observation that presaged future findings in humans.
Starzl reopened the Denver liver program in 1967 and adjusted patient care based on the innovations he had developed. He treated patients with three drugs — azathioprine, steroids, and ALG — and survival times began to exceed one year. The world’s longest survivor has now carried her transplanted liver for more than four decades. Although most in the medical community still considered the procedure too risky, Calne forged ahead to open the second liver transplantation program in 1968.
Full steam ahead
Key advances in immunosuppressive drug regimens further improved organ-transplant outcomes. Calne pioneered the use of the most potent agent yet — cyclosporin A — which he brought to the clinic in the late 1970s. The compound could harm the kidneys, but Starzl ushered it to its full potential by demonstrating that the toxicity could be reduced by combining it with prednisone. Finally, most liver transplant patients were surviving for longer than a year.
In 1983, the US Surgeon General convened a Consensus Development Conference for liver transplantation, which concluded that liver transplantation had progressed past “experimental procedure” status into a “clinical service.” The treatment had finally gained acceptance, and centers worldwide rushed to offer it.
Clinicians continued to seek alternative agents that combat rejection while minimizing adverse side effects. In 1989, Starzl (by then in Pittsburgh) introduced FK506 (Tacrolimus), a compound that differed chemically from existing immunosuppressants, first in individuals who were rejecting organs despite conventional regimens and then in new transplant patients. FK506 gained fast-track US Food and Drug Administration approval in November 1993. Calne next added rapamycin — a chemical that resembles FK506 structurally, but has a different mechanism of action and toxicity profile — to the armamentarium. He also pioneered the use of the powerful monoclonal antibody immunosuppressant, alemtuzumab (Campath), first to treat rejection and then as a pre-emptive therapy to prevent that complication altogether.
Human liver transplantations have not only saved lives, but have provided insights into medical conundrums. In 1969, a liver transplant by Starzl alleviated symptoms of Wilson’s disease, a condition that causes copper accumulation in many tissues, and thus revealed that the illness’s roots lie in the liver. Fifteen years later, Starzl transplanted a liver into a girl with two defective genes for the low-density-lipoprotein (LDL) receptor. Her improved blood LDL profile showed dramatically that this organ houses the receptors that remove cholesterol-carrying LDL from the blood.
Today, liver transplantation has taken hold in sophisticated medical practice across the world, and some patients even survive long-term without medication. In the United States, surgeons use the procedure most commonly to benefit adults who have sustained liver scarring — or cirrhosis — from hepatitis C infection and children who have biliary atresia. More than half of the liver-transplant patients who underwent surgery in 1998 were alive ten years later, and in 2009, almost 50,000 Americans carried a transplanted liver.
Calne and Starzl persevered on a bold course against a backdrop of doubt. By following glints of hope, they have brought new life to thousands of individuals.
by Evelyn Strauss
Key publications of Roy Calne
Calne, R.Y. (1960). The rejection of renal homografts. Inhibition in dogs by 6- mercaptopurine. Lancet. 1, 417-418.
Calne, R.Y. and Williams, R. (1968). Liver Transplantation in man. I. Observations on technique and organization in five cases. Brit. Med. J. 4, 535-540.
Calne, R.Y., Sells, R.A., Pena, J.R., Davis, D.R., Millard, P.R., Herbertson, B.M., Binns, R.M., and Davies, D.A. (1969). Induction of immunological tolerance by porcine liver allografts. Nature. 223, 472-476.
Calne, R.Y. and White, D.J. (1982). The use of cyclosporine A in clinical organ grafting. Ann. Surg. 196, 330-337.
Calne, R.Y., Collier, D.S., Lim, S., Pollard, S.G., Samaan, A., White, D.J.G., and Thiru, S. (1989). Rapamycin for immunosuppression in organ grafting. Lancet. 2, 227.
Calne, R.Y. (2008). Early days of liver transplantation. Am. J. Transplant. 8, 1775-1778.
Key publications of Thomas E. Starzl
Starzl, T.E., Groth, C.G., Brettschneider, L., Penn, I., Fulginiti, V.A., Moon, J.B., Blanchard, H., Martin, A.J. Jr., and Porter, K.A. (1968). Orthotopic homotransplantation of the human liver. Ann. Surg. 168, 392-415.
DuBois, R.S., Rodgerson, D.O., Martineau, G., Shroter, G., Giles, G., Lilly, J., Halgrimson, C.G., Starzl, T.E., Sternlieb, I., and Scheinberg, I.H. (1971). Orthotopic liver transplantation for Wilson’s disease. Lancet. 297, 505-508.
Starzl, T.E., Iwatsuki, S., Van Thiel, D.H., Gartner, J.C., Zitelli, B.J., Malatack, J.J., Schade, R.R., Shaw, B.W. Jr., Hakala, T.R., Rosenthal, J.T., and Porter K.A. (1982). Evolution of liver transplantation. Hepatology. 2, 614-636.
Bilheimer, D.W., Goldstein, J.L., Grundy, S.M., Starzl, T.E., and Brown, M.S. (1984). Liver transplantation to provide low-density-lipoprotein receptors and lower plasma cholesterol in a child with homozygous familial hypercholesterolemia. N. Eng. J. Med. 311, 1658-1664.
Starzl, T.E., Todo, S., Fung, J., Demetris, A.J., Venkataramman, R., and Jain, A. (1989). FK 506 for liver, kidney, and pancreas transplantation. Lancet. 334, 1000-1004.
Starzl, T. E. and Fung, J. J. (2010). Themes of liver transplantation. Hepatology. 51, 1869-1884.
Award presentation by Craig Thomson
 The best in human achievement is often brought out when there are two closely matched rivals, competitors who bring out the best in each other as they strive to succeed. In sports, a number of such historic rivalries come to mind: Mickey Mantle and Roger Maris in baseball, Larry Bird and Magic Johnson in basketball, Mohammed Ali and Joe Frazier in boxing.
The best in human achievement is often brought out when there are two closely matched rivals, competitors who bring out the best in each other as they strive to succeed. In sports, a number of such historic rivalries come to mind: Mickey Mantle and Roger Maris in baseball, Larry Bird and Magic Johnson in basketball, Mohammed Ali and Joe Frazier in boxing.
Today, we honor two physicians who pushed each other to achieve something believed by the medical profession to be impossible. Their rivalry has been just as compelling and competitive as any sports duo, but their combined achievements will have a much more lasting impact.
Acceptance remarks

Acceptance remarks, 2012 Lasker Awards Ceremony
As a medical student in 1950, one of my patients was a boy of my age dying of kidney failure and I was instructed to make him comfortable, for he would be dead in two weeks. I asked if he could have a graft of a kidney, and I was told “no,” and then when I asked “why,” the subject was dismissed with the words “it can’t be done.” A few years later, Dr. Joseph Murray demonstrated that it could be done with the successful transplantation of a kidney between identical twins. For those who did not have an identical twin, graft rejection would interfere with development of this clinical field, and I started to investigate kidney graft survival in experimental animals in the United Kingdom with total-body X-irradiation, which failed miserably. I decided to use anti-leukemia drugs and was fortunate in achieving prolongation of kidney grafts survival in animals treated with 6-mercaptopurine.
I was awarded a Harkness Fellowship at the Peter Bent Brigham Hospital in Dr. Francis Moore’s department and the laboratory of Dr. Joseph Murray. On my way to Boston, I met Drs. Hitchings and Elion, who had synthesized 6-mercaptopurine, and asked them if they had anything better. They gave me some compounds, one of which was azathioprine, which proved to be a little better than 6-mercaptopurine and, when used in the clinic with steroids, was the start of clinical organ transplantation between individuals who were not twins.
On returning to the United Kingdom, I started a program of kidney transplantation and also experimental liver grafting and found, unexpectedly, that pig liver transplants were sometimes not rejected. This ‘liver tolerance’ was a fascinating subject immunologically, and the mechanism has still not been fully determined.
Jean Borel described the immunosuppressive effects of cyclosporine, but the Sandoz company felt it was not worth pursuing. The results we obtained with cyclosporine on organ grafts were better than any other immunosuppressive regimen. With some difficulty, I persuaded Sandoz to produce the compound in sufficient amount to investigate in the clinic. Unexpected nephrotoxicity was observed, but when the dosage was carefully adjusted, cyclosporine changed the one-year functional survival of kidney grafts from 50% to 80%. This was a watershed in organ transplantation; prior to this, approximately ten centers in the world were seriously involved. Within two years after the introduction of cyclosporine to the clinic, there were more than 1000.
I started the clinical liver transplant program in Cambridge in 1968 and had frequent contacts with Dr. Starzl so that we could learn from each other’s experience and try to avoid making the same mistakes.
In Cambridge, we developed rapamycin, which proved to be an effective immunosuppressant but had a completely different mode of action to the calcinurine inhibitors and on its own had little or no nephrotoxicity.
Using the powerful monoclonal antibody produced by Waldmann’s group in Cambridge, campath-1H, we started a program of preemptive induction with the antibody at the time of operation and then minimal maintenance drug dosage, half of one drug instead of full dose of three. This we called “almost” or “prope tolerance.”
We can expect continuing advances, but also it is necessary to address the ethical dilemmas raised by transplantation where the generosity and charity of the donor must not be abused due to the shortage of organ donors.
The priceless reward for successful liver transplantation has been the outstanding quality of life that many of the patients have achieved. My longest survivor at 38 years has recently completed a 150-mile hill cycle ride. I found that painting some of my patients enabled me to establish personal friendships and, with children, drove away the fear of a doctor in a white coat.
Acceptance remarks, 2012 Lasker Awards Ceremony
Thank you for this award — and for the bonus of a reunion with my old and deserving friend, Roy Calne. When we arrived on the scene 50 years ago, patients dying from end-stage kidney, liver, or other vital organ diseases could be offered little more than priestly comfort.
The thrilling concept of organ replacement that then began to take shape was a beacon of hope. However, the technology could not be efficiently applied until rejection could be reliably controlled.
Once that was accomplished, all decisions in the care of patients with failure of a vital organ would have to take into account the possibility of transplantation. Nowhere was this more clear than with end-stage hepatic diseases for which transplantation up to the present day is the only option.
As transplantation of different kinds of organs was accomplished, thoughts turned back to what might have been. How much more complete would the world have been if Mozart could have received a kidney transplant instead of dying of glomerulonephritis at the age of 35? A generation later, Beethoven died of liver disease. Or closer to home, what might have become of our friend turned blue by heart disease, who stopped coming to classes one day and never was seen again?
Transplantation has not previously been acknowledged by a Lasker prize. One reason could be the difficulty of determining who should get it. Transplantation services are not provided by single individuals. The team is what counts, and it is on behalf of my research and clinical teams — first in Denver and then in Pittsburgh — that I accept this prize.
And by the way, the prize could have gone to one of those courageous kidney, liver, or heart recipients who faced the great unknown in the early years and chose to run the uncharted gauntlet of transplantation instead of giving up. Win or lose, these were the heroes. Some of the winners are in this room today.
Very few people have been privileged to see their grand illusion mature into reality. Sir Roy Calne and I were amongst those exceptions, beginning a half-century ago. That means, of course, that we are just about the oldest people in this room today. The fine lunch and all that goes with it are cherished rewards.
Interview with Roy Calne and Thomas E. Starzl
Video Credit: Susan Hadary
