
Akira Endo
Biopharm Research Laboratories, Inc.
For the discovery of the statins — drugs with remarkable LDL-cholesterol-lowering properties that have revolutionized the prevention and treatment of coronary heart disease.
The 2008 Lasker~DeBakey Award for Clinical Medical Research honors a scientist who discovered statins — drugs with remarkable LDL-cholesterol-lowering properties that have revolutionized the prevention and treatment of coronary heart disease (CHD). Akira Endo (Biopharm Research Laboratories, Inc., Tokyo) sifted through thousands of organisms, hunting for natural substances that block a key enzyme in the biochemical pathway that produces cholesterol, a major contributor to CHD. Remarkably, the compound that Endo found lowers concentrations of LDL (the bad cholesterol) but not HDL (the good cholesterol) in the bloodstream of animals and humans. His work stimulated Merck, Sharp & Dohme Research Laboratories (Merck) to launch a drug-development program that led, 20 years ago, to the first statin approved for medical use. This advance paved a path for other pharmaceutical companies to follow.
LDL in the bloodstream can form fatty deposits that narrow blood vessels. When this process occurs in arteries that deliver blood to the heart, it can lead to CHD, the major cause of chest pain and heart attack and the top killer in the industrialized world. In the US, more than 450,000 people died from CHD in 2004. In 2005, the American Heart Association estimated that 16 million Americans had CHD and 1.2 million would have a new or recurrent heart attack that year. Statin use is increasing — 30 million people worldwide are taking them — and has begun to make a dent in those numbers. The drugs dramatically reduce the risk of CHD and its associated life-threatening events. Furthermore, studies with statins have erased long-standing doubt about the possibility of safely reducing cholesterol quantities with pharmaceutical agents.
Promising early results
In the 1950s and 1960s, epidemiological studies suggested a link between LDL cholesterol in the blood and CHD. Reducing LDL would shrink the incidence of this illness, some experts reasoned. However, many scientists and clinicians questioned whether doing so would stir trouble. Cholesterol is a crucial component of the membranes that encase our cells, and it serves as a raw material for other essential molecules, including some hormones and the sheath that insulates nerves. Further exacerbating uncertainty, most early agents that reduced cholesterol quantities in the blood cut concentrations only modestly and triggered unwelcome side effects. Therefore, skepticism simmered about the wisdom of lowering cholesterol concentrations.
Despite the concerns, efforts pushed forward. Humans acquire cholesterol from food and we also make it in our bodies, mostly in the liver. Dietary interventions to limit cholesterol intake had met with poor success and the idea of short-circuiting our ability to produce the compound seemed attractive. An enzyme called HMG-CoA reductase plays a central role in the manufacture of cholesterol. In the biochemical pathway that generates cholesterol, it converts a precursor molecule, HMG-CoA, into the next compound, mevalonate.
By 1971, when Endo began his work (at Sankyo Company in Tokyo), thwarting the reductase seemed like a possible way to keep the body’s cholesterol production in check. Endo had a novel idea about how to find substances that block the reductase. Aware that organisms can secrete compounds with powerful biological activities — presumably to kill their competitors — Endo proposed that some creatures might spit out chemicals that foil the reductase and thus impede a vital activity of their neighbors.
Over the next two years, Endo and colleagues grew more than 6000 fungi, harvested the broth in which each had grown, and tested whether the material could interfere with an early step of cholesterol synthesis in a test tube. They then separated its components from one another, keeping track of the active material. By this and additional methods, he purified a substance from the fungus Penicillium citrinum, called mevastatin or compactin, that blocks the reductase.
Additional analysis revealed that compactin resembles HMG-CoA and competes strongly with it for the site on the enzyme that catalyzes HMG-CoA’s conversion to mevalonate. This capacity to bind specifically to the spot normally reserved for the enzyme’s substrate suggested that the potential drug would not randomly clasp molecules in cells and disrupt other important activities.
Endo wondered whether compactin would reduce enzyme activity in animals, as it does in test tubes. In 1979, he showed that the compound dramatically lowers blood cholesterol in dogs and monkeys with no obvious toxic effects.
While these results were coming in, Endo and physician Akira Yamamoto (National Cardiovascular Center in Osaka) gave compactin to patients with extremely high LDL-cholesterol levels. In 1980, they reported that it cut LDL in the blood by an average of 27%. The next year, Hiroshi Mabuchi of Kanazawa School of Medicine published similarly promising findings. Furthermore, he established that the compound did not perturb quantities of a molecule that is involved in the cell’s energy-production system whose concentrations experts thought might drop when HMG-CoA activity was stymied. These observations fed hope that compactin could reduce cholesterol without causing harm.
At the same time, different researchers were demonstrating the mechanism by which the drug acted, which provided a rationale for how it could operate safely. In 1974, Michael Brown and Joseph Goldstein (Lasker Basic Medical Research Award and Nobel Prize, 1985) at the University of Texas Southwestern Medical School discovered that cell-surface molecules known as LDL receptors on liver cells grab LDL in the blood. In 1981, they showed that, when statins lower reductase activity and cholesterol production wanes, cells place additional LDL receptors on their surfaces. Statins thus harness a normal mechanism by which cells drain cholesterol from the blood, yet ensure a steady supply of the molecule internally for vital activities.
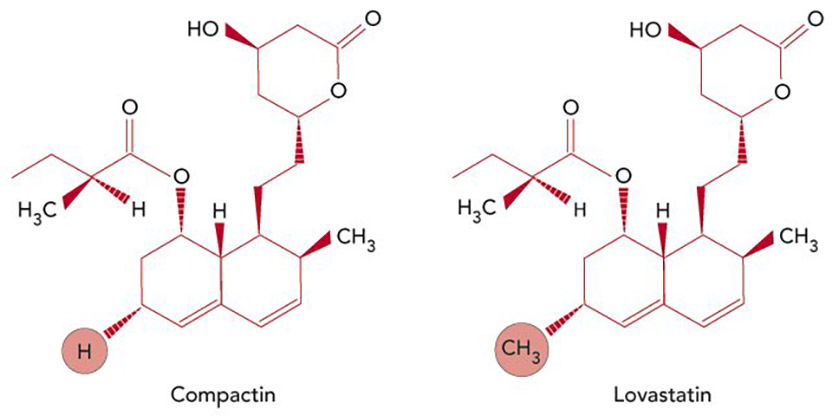
Reducing cholesterol. Compactin, the first statin, discovered by Akira Endo (left); Lovastatin, the first statin approved for clinical use, developed by Merck (right). The compounds differ by a single methyl group at the circled position. [Credit: Carin Cain]
Statins in the clinic
In 1978, Endo left Sankyo and joined the faculty of Tokyo University of Agriculture and Technology. There, he isolated additional HMG-CoA reductase inhibitors, including one called monacolin K, from another fungus. Merck scientists, led by Alfred W. Alberts, independently identified — from a different organism — the same compound, which they called mevinolin (and subsequently renamed lovastatin). The company had been pursuing statin-related research since soon after Endo published his first papers in 1976. At that time, P. Roy Vagelos, then President of Merck Research Laboratories, had signed an agreement with Sankyo and obtained samples of compactin from Endo, with which Merck confirmed Endo’s results and launched its own program.
In April 1980, Merck began clinical studies of lovastatin. Several months later, rumors emerged from Sankyo that its drug (compactin) caused tumors in dogs. Because of this uncertainty, Merck halted the studies of its drug (lovastatin). However, experts in the field urged Merck forward. The dogs at Sankyo were receiving exceptionally high doses of compactin and Sankyo provided no data for others to assess. Japanese investigators were witnessing dramatic benefits with compactin, particularly to individuals who have a genetic alteration in one of their two copies of the gene for the LDL receptor and thus carry colossal quantities of circulating cholesterol; these patients are extremely difficult to treat.
Several years later, Merck picked up its clinical trials on lovastatin. In 1987, the FDA approved the drug (Mevacor®).
The success of compactin and lovastatin inspired efforts to improve the statins by chemically modifying the natural compounds or crafting synthetic ones. Because the statins curb LDL so much more than any of the existing treatments, it became possible to demonstrate unequivocally that the drugs decrease CHD events without serious side effects. For example, in 1994, the Scandinavian Simvastatin Survival Study (4S study) showed that treatment with simvastatin (the second Merck statin) — for as short a period as 5 years — lowered LDL levels by 35%; this reduction was associated with a drop of 40% in CHD deaths. A 2005 analysis of more than 90,000 people in multiple 5-year randomized studies obtained similar results. Furthermore, this work established that people reap these benefits without an increase in cancer, other diseases, or deaths from any cause.
Statins are now routinely used to prevent and treat CHD throughout the world. Although CHD is aggravated by multiple risk factors in addition to high LDL — cigarette smoking, high blood pressure, obesity, and diabetes — reducing LDL levels alone makes a significant impact.
By discovering statins, Endo ushered in a new era in preventing and treating CHD, the leading cause of death in the US and a major source of human suffering. His work has touched millions of people and promises to prolong and improve the lives of many millions more.
by Evelyn Strauss
Key publications of Akira Endo
Endo, A., Kuroda, M., and Tanzawa, K. (1976). Competitive inhibition of 3-hydroxy-3-methylglutaryl coenzyme A reductase by ML-236A and ML-236B fungal metabolites, having hypocholesterolmic activity. FEBS Lett. 72, 323-326.
Endo, A., Kuroda, M., and Tsujita, Y. (1976). ML-236A, ML-236B, and ML-236C, new inhibitors of cholesterogenesis produced by Penicillium citrinium. J. Antibiot. (Tokyo). 29, 1346-1348.
Endo, A., Tsujita, Y., Kuroda, M., and Tanzawa, K. (1977). Inhibition of cholesterol synthesis in vitro and in vivo by ML-236A and ML-236B, competitive inhibitors of 3-hydroxy-3-methylglutaryl-coenzyme A reductase. Eur. J. Biochem. 77, 31-36.
Tsujita, Y., Kuroda, M., Tanzawa, K., Kitano, N., and Endo, A. (1979). Hypolipidemic effects in dogs of ML-236B, a competitive inhibitor of 3-hydroxy-3-methylglutaryl coenzyme A reductase. Atherosclerosis. 32, 307-313.
Yamamoto, A., Sudo, H., and Endo, A. (1980). Therapeutic effects of ML-236B in primary hypercholesteromia. Atherosclerosis. 35, 259-266.
Endo, A. (1992). The discovery and development of HMG-CoA reductase inhibitors. J. Lipid Res. 33, 1569-1582.
Award presentation by Joseph Goldstein
 The human body produces tens of thousands of different molecules. Several of them — DNA, hemoglobin, insulin, estrogen — are household names. But none has captured the public’s imagination like cholesterol. Cholesterol is the quintessential celebrity molecule: it appears regularly on the front pages of USA Today and the New York Times, on the covers of Time and Newsweek, and it’s the subject of endless Jay Leno jokes, New Yorker cartoons, and cocktail party conversations. Many of you in the room know your cholesterol level but can’t remember your wedding anniversary.
The human body produces tens of thousands of different molecules. Several of them — DNA, hemoglobin, insulin, estrogen — are household names. But none has captured the public’s imagination like cholesterol. Cholesterol is the quintessential celebrity molecule: it appears regularly on the front pages of USA Today and the New York Times, on the covers of Time and Newsweek, and it’s the subject of endless Jay Leno jokes, New Yorker cartoons, and cocktail party conversations. Many of you in the room know your cholesterol level but can’t remember your wedding anniversary.
Acceptance remarks by Akira Endo

Acceptance remarks, 2008 Lasker Awards Ceremony
It is a great honor for me to receive the 2008 Lasker Award in Clinical Medical Research. I thank the members of the jury and the foundation that made it possible.
Four decades ago, from 1966 to 1968, I studied at the Albert Einstein College of Medicine here in New York. Even before that time I was interested in cholesterol metabolism, and during my stay here, I learnt much about cholesterol both in my daily work and life.
Interview with Akira Endo
Video Credit: Susan Hadary
